A Brief History of UHS Lifelines
UHS Lifelines owes its origins to concept work by a team at the Human Computer Interaction Laboratory (HCIL) at the University of Maryland, Washington DC, in the mid 1990s, under the leadership of Professor Ben Shneiderman.
Figure 1. A life of crime: The evolving criminal career of Bart Simpson: read more from the Human Computer Interaction Laboratory, University of Maryland
Between 1994 and 1996, the HCIL team at the University of Maryland were commissioned to develop an overview system to organise the flows of information around the evolving criminal careers of young people: read about the Maryland Dept of Juvenile Services.
Their data visualisation model, which they called Lifelines, is illustrated in their plot of Bart Simpson’s early criminal career (Figure 1).
This work evolved into a wider study into the information architecture required to support the visualisation of the types of personal histories, and then into a concept model for clinical information in primary health care.
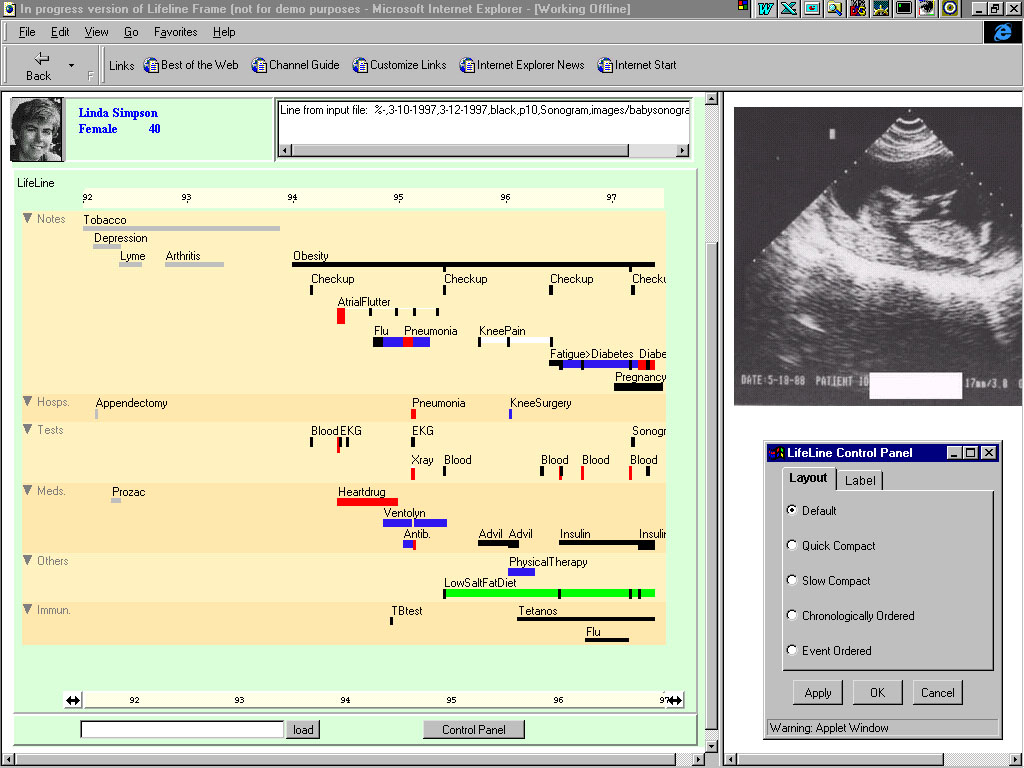
Figure 2. The HCIL Maryland Lifelines EPR model interface from the Human Computer Interaction Laboratory, University of Maryland
The key features of the Lifelines concept are:
– The computerisation of the entire data set, which allows a wide range of interactions with the core data, and dynamic changes in the X and Y axes with time and content
– The series of stacked, parallel timelines on the Y axis, on which each timeline represents a different subject field
– The placement of dynamic (interactive) icons on the timelines, which allows the direct opening of specific documents and images.
These concept designs did not evolve into working clinical versions at that time, and there was little follow through of this very elegant concept in the international literature.
UHS Lifelines comes to Southampton
By 2009, it was clear in Southampton that a new approach was needed to accommodate large quantities of clinical data in the evolving Electronic Patient Record (EPR). There was a need to optimise the display of the growing volume of documents and reports in the UHS Clinical Data Environment (CDE), for which tab and list mode access in legacy software screen formats was becoming increasingly unsatisfactory.
A wide ranging search of the Internet and of available commercial systems revealed no suitable system which would match the powerful concepts which were expressed in the HCIL Maryland Lifelines model.
Following an examination of the options through the UHS IT Department, we formed a small team to undertake a “blue skies” project to explore and develop our novel EPR concept. This was based around the Maryland Lifelines model.
Key members of the team were Alan Hales, who works as an independent IT Systems Consultant to UHS, and who had also been the software architect of key elements of the UHS CDE (including HICSS, e-Quest and eDocs); and David Cable, who facilitated the project for the UHS IT team.
Traditional software development is known as waterfall development, though which software developers work to a strictly prescribed design template which has been written in advance. This template mandates a very clear understanding of the final product, which is very rarely achievable in high complex and rapidly changing data environments such as define a large University Hospital. Waterfall software development costs are high, and the costs of failure of waterfall projects can and have been exorbitant for the NHS.
The alternative approach to software development, which has been championed since 2010 by the UK Government Digital Service (GDS), is the Agile methodology. In the agile software development process, the developers work closely with User Experience (UX) assessors and the true end users to understand their precise needs and to adapt the software directly to those needs.
The agile process works through a series of short, iterative development cycles or “sprints”, which test and modify the evolving software against the user needs. This iterative, “fail early, fail fast” approach speeds up the development cycle, while eliminating most of the costs of bad design and un-usability.
Agile development produces “digital by default” software which is optimised for end user satisfaction, rather than “digital by diktat” software, which obliges disgruntled and non-engaged users to use poorly designed and inefficient software.
The UHS Lifelines Agile Development Approach
Using the HCIL Lifelines concept as a broad template for our curiosity driven research and development, we worked in a very agile way to no specific blueprint, and with no designated funding or external resources, to create the first working version of Lifelines (UHS Lifelines V1.0) within the digital test environment at UHS.
By September 2010, we were able to demonstrate UHS Lifelines V1.0 to the Trust, and the system was awarded an NHS Regional Innovations Award in November 2011 (Figure 3).
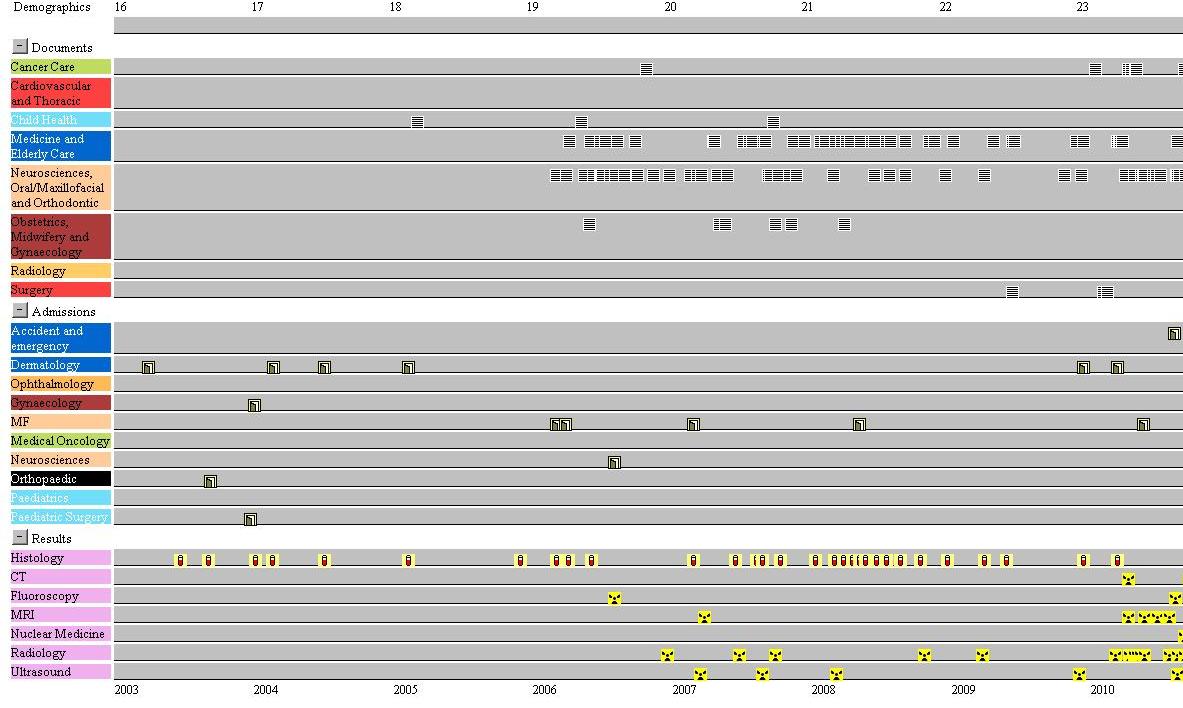
Figure 3. UHS Lifelines v1.0 (September 2010). This is a live screenshot of a young person with multiple complex and severe co-morbidities since birth.
UHS Lifelines v 1.0 differed from the original HCIL Maryland Lifelines model in various ways.
– It was built on live data
– it included a collapse/expand (+/-)Y axis of documents, results and admissions to accommodate a growing number of timelines on the screen
– it eliminated horizontal bars to display continuous information (eg for medication use)
– it eliminated in line text descriptors.
The net result was a very clean interface, with which we were able to confirm the UHS lifelines proof of concept. We were able to display and interact with the entire documentary EPR on a single desktop screen in a live hospital data environment, and we believe this to have been the first ever working integrative and interactive EPR of its kind.
In 2010, the unitary UHS CHARTS EPR had not been built, and for various reasons UHS Lifelines was not adopted into mainstream use at that time. Nevertheless, development continued within the UHS Surgical Breast Service, where it became a key component of the similarly innovative UHS Breast Cancer Data System.
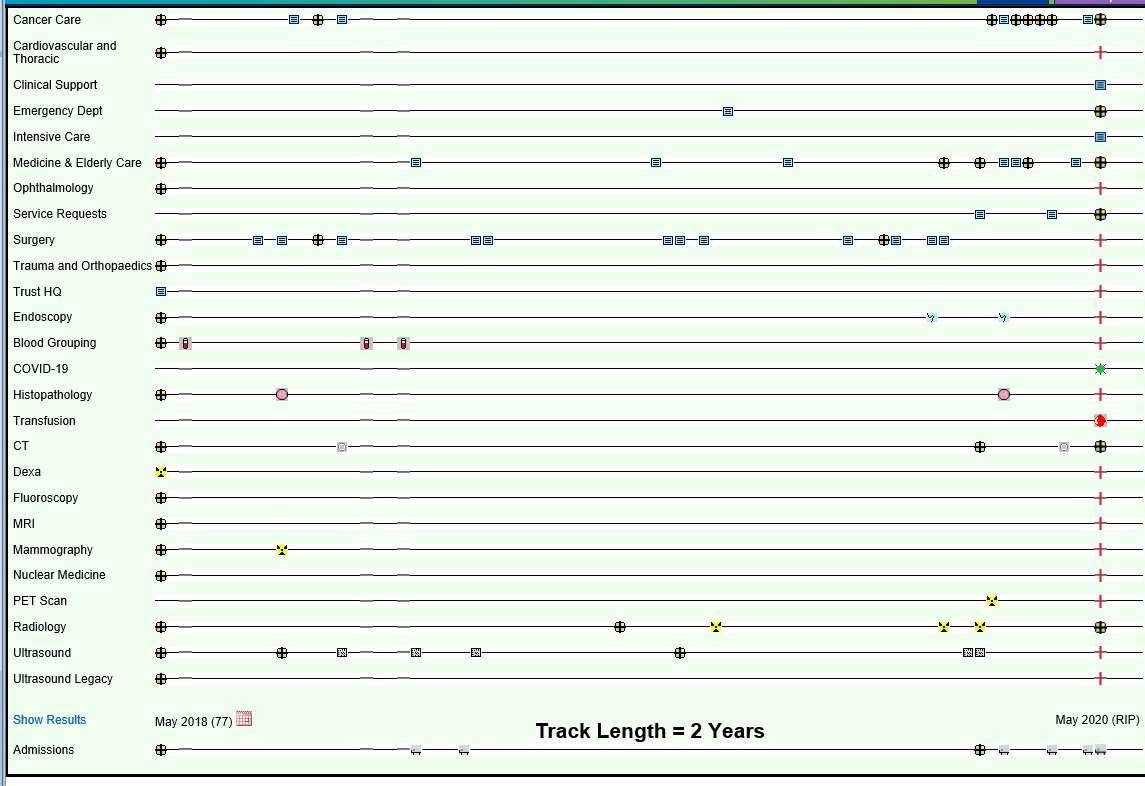
Figure 4. This illustrates a recent UHS Lifelines screenshot (May 2020) of a patient with multiple co-morbidities, and with a range of design changes since V1.0 in 2010. Note the adaptability of the design with the inclusion of the Covid19 timeline, with a green “virus” icon to show that the patient was antigen negative at the time of testing.
From 2010 to 2016, UHS Lifelines progressed through a series of agile iterations and code rewrites, in parallel with the integration of a number of other EPR components (eDocs, eQuest, e-Camis) into the new primary EPR framework, CHARTS, in late 2016.
In future blog posts in this series, we will examine in greater detail a number of evolved design features which enhance the usability and the potential for further exploitation of the system.
David Rew
Consultant General Surgeon
University Hospital Southampton
UHS Lifelines Concept Lead